0 items
No products in the cart.

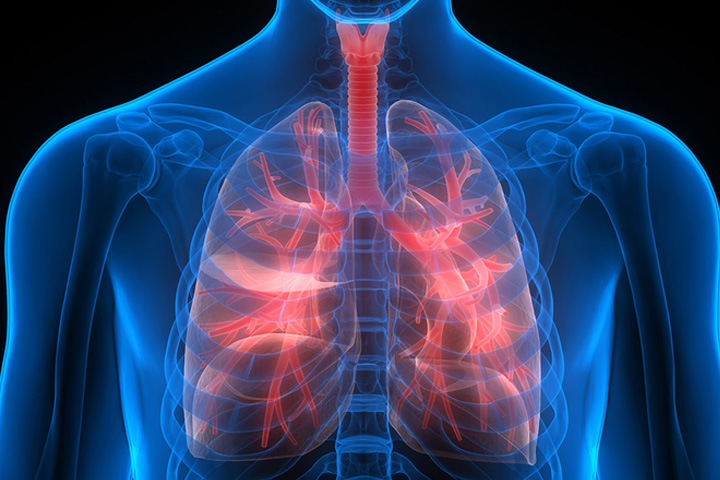
What is COPD?
Chronic obstructive pulmonary disease (COPD),is the occurrence of chronic bronchitis or emphysema, a pair of commonly co-existing diseases of the lungs in which the airways become narrowed. This leads to a limitation of the flow of air to and from the lungs, causing shortness of breath (dyspnea). In clinical practice, COPD is defined by its characteristically low airflow on lung function tests. In contrast to asthma, this limitation is poorly reversible and usually gets progressively worse over time. In England, an estimated 842,100 of 50 million people have a diagnosis of COPD.
COPD is caused by noxious particles or gas, most commonly from tobacco smoking, which triggers an abnormal inflammatory response in the lung. The diagnosis of COPD requires lung function tests. Important management strategies are smoking cessation, vaccinations, rehabilitation, and drug therapy (often using inhalers). Some patients go on to require long-term oxygen therapy or lung transplantation.
Worldwide, COPD ranked as the sixth leading cause of death in 1990. It is projected to be the fourth leading cause of death worldwide by 2030 due to an increase in smoking rates and demographic changes in many countries.[5] COPD is the third leading cause of death in the U.S. and the economic burden of COPD in the U.S. in 2007 was $42.6 billion in health care costs and lost productivity.
What is Chronic bronchitis?
Lung damage and inflammation in the large airways results in chronic bronchitis. Chronic bronchitis is defined in clinical terms as a cough with sputum production on most days for 3 months of a year, for 2 consecutive years. In the airways of the lung, the hallmark of chronic bronchitis is an increased number (hyperplasia) and increased size (hypertrophy) of the goblet cells and mucous glands of the airway. As a result, there is more mucus than usual in the airways, contributing to narrowing of the airways and causing a cough with sputum.
Inflammation is followed by scarring and remodeling that thickens the walls and also results in narrowing of the airways. As chronic bronchitis progresses, there is squamous metaplasia (an abnormal change in the tissue lining the inside of the airway) and fibrosis (further thickening and scarring of the airway wall). The consequence of these changes is a limitation of airflow.
What is Emphysema?
Lung damage and inflammation of the air sacs (alveoli) will result in emphysema. Emphysema is defined as enlargement of the air spaces distal to the terminal bronchioles, with destruction of their walls. The destruction of air space walls reduces the surface area available for the exchange of oxygen and carbon dioxide during breathing. It also reduces the elasticity of the lung itself, which results in a loss of support for the airways that are embedded in the lung. These airways are more likely to collapse causing further limitation to airflow.
Signs and symptoms
One of the most common symptoms of COPD is shortness of breath (dyspnea). People with COPD commonly describe this as: “My breathing requires effort,” “I feel out of breath,” or “I can’t get enough air in”. People with COPD typically first notice dyspnea during vigorous exercise when the demands on the lungs are greatest. Over the years, dyspnea tends to get gradually worse so that it can occur during milder, everyday activities such as housework. In the advanced stages of COPD, dyspnea can become so bad that it occurs during rest and is constantly present.
Other symptoms of COPD are a persistent cough, sputum or mucus production, wheezing, chest tightness, and tiredness.[17][18]
People with advanced (very severe) COPD sometimes develop respiratory failure. When this happens, cyanosis, a bluish discoloration of the lips caused by a lack of oxygen in the blood, can occur. An excess of carbon dioxide in the blood can cause headaches, drowsiness or twitching (asterixis). A complication of advanced COPD is cor pulmonale, a strain on the heart due to the extra work required by the heart to pump blood through the affected lungs.
There are a few signs of COPD that a healthcare worker may detect although they can be seen in other diseases. Some people have COPD and have none of these signs. Common signs are:
Cause
Smoking:
The primary risk factor for COPD is chronic tobacco smoking. In the United States, 80 to 90% of cases of COPD are due to smoking. Exposure to cigarette smoke is measured in pack-years, the average number of packages of cigarettes smoked daily multiplied by the number of years of smoking. The likelihood of developing COPD increases with age and cumulative smoke exposure, and almost all life-long smokers will develop COPD, provided that smoking-related, extrapulmonary diseases (cardiovascular, diabetes, cancer) do not claim their lives beforehand.
Air pollution:
Studies in many countries have found people who live in large cities have a higher rate of COPD compared to people who live in rural areas. Urban air pollution may be a contributing factor for COPD, as it is thought to slow the normal growth of the lungs, although the long-term research needed to confirm the link has not been done. Studies of the industrial waste gas and COPD/asthma-aggravating compound, sulfur dioxide, and the inverse relation to the presence of the blue lichen Xanthoria (usually found abundantly in the countryside, but never in towns or cities) have been seen to suggest combustive industrial processes do not aid COPD sufferers.
Management
There is currently no cure for COPD; however, COPD is both a preventable and treatable disease. Clinical practice guidelines for the management of COPD are available from the Global Initiative for Chronic Obstructive Lung Disease (GOLD), a collaboration that includes the World Health Organization and the U.S. National Heart, Lung, and Blood Institute. The major current directions of COPD management are to assess and monitor the disease, reduce the risk factors, manage stable COPD, prevent and treat acute exacerbations and manage comorbidity.
The only measures that have been shown to reduce mortality is smoking cessation and supplemental oxygen.
Supplemental oxygen:
Supplemental oxygen can be given to people with COPD who have low oxygen levels in the body. Oxygen is provided from an oxygen cylinder or an oxygen concentrator and delivered to a person through tubing via a nasal cannula or oxygen mask. Supplemental oxygen does not greatly improve shortness of breath but can allow people with COPD and low oxygen levels to do more exercise and household activity. Long-term oxygen therapy for at least 16 hours a day can improve the quality of life and survival for people with COPD and arterialhypoxemia or with complications of hypoxemia such as pulmonary hypertension, cor pulmonale, or secondaryerythrocytosis.[56] High concentrations of supplemental oxygen can lead to the accumulation of carbon dioxide and respiratory acidosis for some people with severe COPD; lower oxygen flow rates are generally safer for these individuals. Another safety issue concerning the use of oxygen for patients with COPD is smoking, because the combination of smoking and oxygen can result in fire accidents. Nowadays oxygen is generally only given to patients who have stopped smoking.
Other measures
Pulmonary rehabilitation is a program of exercise, disease management and counselling coordinated to benefit the individual. Pulmonary rehabilitation has been shown to improve shortness of breath and exercise capacity. It has also been shown to improve the sense of control a patient has over their disease as well as their emotions.
Being either underweight or overweight can affect the symptoms, degree of disability and prognosis of COPD. People with COPD who are underweight can improve their breathing muscle strength by increasing their calorie intake. When combined with regular exercise or a pulmonary rehabilitation programme, this can lead to improvements in COPD symptoms.
Surgery is sometimes helpful for COPD in selected cases. A bullectomy is the surgical removal of a bulla, a large air-filled space that can squash the surrounding, more normal lung. Lung volume reduction surgery is similar; parts of the lung that are particularly damaged by emphysema are removed allowing the remaining, relatively good lung to expand and work better. Lung transplantation is sometimes performed for severe COPD, particularly in younger individuals.
Patients should be given annual influenza vaccinations and pneumococcal vaccinations if appropriate. Obesity, poor nutrition, depression and social isolation are looked at. Palliative care for end of life needs is important. Morphine and benzodiazepines are used in low doses to reduce anxiety. In advanced critical illness, decisions about resuscitation are addressed.
Lung cancer
Lung cancer is a disease characterized by uncontrolled cell growth in tissues of the lung. If left untreated, this growth can spread beyond the lung in a process called metastasis into nearby tissue and, eventually, into other parts of the body. Most cancers that start in lung, known as primary lung cancers, are carcinomas that derive from epithelial cells. The main types of lung cancer are small cell lung carcinoma (SCLC), also called oat cell cancer, and non-small cell lung carcinoma (NSCLC). The most common cause of lung cancer is long-term exposure to tobacco smoke. Nonsmokers account for 15% of lung cancer cases, and these cases are often attributed to a combination of genetic factors, radon gas, asbestos, and air pollution including secondhand smoke.
The most common symptoms are coughing (including coughing up blood), weight loss and shortness of breath. Lung cancer may be seen on chest radiograph and computed tomography (CT scan). The diagnosis is confirmed with a biopsy. This is usually performed by bronchoscopy or CT-guided biopsy. Treatment and prognosis depend on the histological type of cancer, the stage (degree of spread), and the patient’s general wellbeing, measured by performance status. Common treatments include surgery, chemotherapy, and radiotherapy. NSCLC is sometimes treated with surgery, whereas SCLC usually responds better to chemotherapy and radiation therapy. This is partly because SCLC often spreads quite early, and these treatments are generally better at getting to cancer cells that have spread to other parts of the body.
Survival depends on stage, overall health, and other factors, but overall 15% of people in the United States diagnosed with lung cancer survive five years after the diagnosis. Worldwide, lung cancer is the most common cause of cancer-related death in men and women, and is responsible for 1.3 million deaths annually, as of 2004.
Signs and symptoms
If the cancer grows in the airway, it may obstruct airflow, causing breathing difficulties. The obstruction can lead to accumulation of secretions behind the blockage, and predispose to pneumonia. Many lung cancers have a rich blood supply. The surface of the cancer may be fragile, leading to bleeding from the cancer into the airway. This blood may subsequently be coughed up.
Many of the symptoms of lung cancer (bone pain, fever, and weight loss) are nonspecific; in the elderly, these may be attributed to comorbid illness. In many patients, the cancer has already spread beyond the original site by the time they have symptoms and seek medical attention. Common sites of metastasis include the brain, bone, adrenal glands, contralateral (opposite) lung, liver, pericardium, and kidneys. About 10% of people with lung cancer do not have symptoms at diagnosis; these cancers are incidentally found on routine chest radiograph.
Heart Failure
How It Works:
Oxygen therapy is a way to get more oxygen into your lungs and bloodstream. It is sometimes used for people who have diseases that make it hard to breathe, such as heart failure. Oxygen therapy can make it easier to breathe. And it can reduce the heart’s workload.
Some people need extra oxygen all the time. Others need it from time to time throughout the day or overnight. A doctor will prescribe how much oxygen you need, based on blood tests. He or she will tell you how much oxygen to use per minute (the flow rate) and how often to use it.
To breathe the oxygen, most people use a nasal cannula (say “KAN-yuh-luh”). This is a thin tube with two prongs that fit just inside your nose. Children and people who need a lot of oxygen may need to use a mask that fits over the nose and mouth.
You don’t have to stay at home or in a hospital to use oxygen. Oxygen systems are portable. You can use them while you do your daily tasks.
Why It Is Used:
Your doctor will determine how much oxygen you need with a blood test called arterial blood gas and another test called oximetry. These tests measure the levels of oxygen in the blood.
Long-term oxygen therapy is given to people with heart failure who have low levels of oxygen in their blood. It is given to increase the amount of oxygen in the blood to provide for the body’s needs.
Oxygen therapy can decrease shortness of breath and allow you to do more.
How Well It Works:
Oxygen therapy helps reduce the heart’s workload. In heart failure, the heart does not pump as effectively as it should and does not meet the body’s needs for oxygen. Oxygen therapy helps compensate by increasing the amount of oxygen delivered to the body’s tissues. Home oxygen therapy can help decrease shortness of breath and increase your capacity to exercise.
Side Effects:
In general, there are no adverse effects from oxygen treatment. But oxygen is a fire hazard. It is important to follow safety measures to keep you and your family safe. Do not use oxygen around lit cigarettes, open flames, or flammable substances.
Your doctor will set the flow rate per minute to give you the right amount of oxygen. Don’t change the flow rate unless your doctor tells you. Higher flow rates usually do not help and can increase the risk of harmful carbon dioxide buildup in the blood, especially in those people who also have lung disease.
See Drug Reference for a full list of side effects. (Drug Reference is not available in all systems.)
What To Think About:
Do not use oxygen around lit cigarettes, open flames, or flammable products. If you or those who care for you smoke, be sure to consider oxygen therapy very carefully because of the danger of fire or explosion.








Compass Medical is a distributor of leading edge medical technologies. Our partners are Philips Healthcare, Bosch Healthcare, Air Liquide, Trudell Medical International, Schiller, Inogen, Restech, Pulmonx and etc.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
COMPASS MEDICAL SDN BHD MALAYSIA
Reg No: 933668P
Registered with Medical Device Authority MDA MALAYSIA
Reg No: MDA-2071-WDP121
Registered with Ministry Of Health MOH MALAYSIA
Reg No: KP6381123915
Registered with Ministry Of Finance MOF MALAYSIA
Reg No: K22098729211788166
GDPMD certification by TUV NORD
Reg No: 22221003
COMPASS MEDICAL's products are reimbursable by JPA
COMPASS MEDICAL's products are reimbursable by KWSP